This is a partial annotated transcript of Dr Peter McCullough testifying on 19 Nov 2020 before the Senate Homeland Security Committee Hearing on COVID-19 Outpatient Treatment. 18 Sep 2021: Up to recently, before he was black-balled for speaking out, Dr McCullough was the Vice Chair of Internal Medicine at Baylor University Medical Center and a Professor of Medicine at Texas A&M College of Medicine. Source of this recording: https://www.c-span.org/video/?478159-1/senate-hearing-covid-19-outpatient-treatment.
Peter A. McCullough, MD, MPH, FACC, FCCP, FAHA, FNKF, FNLA, FCRSA is board certified by the American Board of Internal Medicine in internal medicine and cardiovascular disease. He has extensive training and expertise in lipidology and echocardiography. He holds additional certifications from the American Board of Clinical Lipidology and the National Board of Echocardiography. Dr. McCullough specializes in treating patients with complicated internal medicine problems that have affected important organs including the heart and kidneys. After receiving a bachelor’s degree from Baylor University, Dr. McCullough completed his medical degree as an Alpha Omega Alpha graduate from the University of Texas Southwestern Medical School in Dallas. He went on to complete his internal medicine residency at the University of Washington in Seattle, a cardiology fellowship including service as Chief Fellow at William Beaumont Hospital, and a master’s degree in public health at the University of Michigan. Dr. McCullough oversees cardiology training, education, and research for Baylor Health Care System and is Vice Chief of Medicine at Baylor University Medical Center at Dallas. He is an internationally recognized authority in his field and frequently lectures on internal medicine, nephrology, and cardiology. In addition, he has published over a thousand related scientific communications. He is currently serving as the chair of the National Kidney Foundation’s Kidney Early Evaluation Program, the largest community screening effort for chronic diseases in America. As both a primary care physician and specialist, Dr. McCullough welcomes patients with complicated internal medicine problems that have affected important organs including the heart and kidneys. He is knowledgeable about the roles of diet and exercise in health and disease and commonly provide guidance concerning dietary supplements and treatments for obesity. He has an intimate practice style with frequent patient contact and 24 X 7 access for questions and help with medical problems. His practice involves both teaching and research, therefore, his patients are among the first to have new tests and treatments for high cholesterol, high blood pressure, diabetes, and heart and kidney disease.
Beginning at 4:26:
Senator Ben Johnson (R-WI):
This hearing is not about promoting any one particular therapy over others although as a quick aside by reading the testimony and watching the tweets it may be unavoidable but I have to say, the absence of any serious NIH study or consideration of hydroxychloroquine, either by itself or in combination with other drugs and supplements, is worth discussing. This is a drug that has been safely and effectively used to prevent malaria and treat lupus and rheumatoid arthritis for decades yet doctors who have had the courage to follow the Hippocratic Oath and use their off-label prescription rights to treat patients using hydroxychloroquine have been scorned and state medical boards have threatened to withdraw their licenses. The same has happened to pharmacists filling prescriptions for the drug in some states. Will those using Ivermectin or other off-the-shelf drugs being used off-label to treat covid patients suffer the same fate?
Since the onset of this pandemic I have publicly advocated for allowing doctors to be doctors, to practice medicine, explore different therapies and share their knowledge within the medical community and with the public. I believe international, federal, and state medical agencies and institutions have let us down. I fear too many have been close-minded bureaucrats, potentially driven by conflicting interests and agendas. Tragically, media and the social media have failed to ask the right questions and censored what they do not understand. My public advocacy has connected me to doctors who care and who are trying to compassionately help their patients in spite of the bureaucratic roadblocks that they’ve encountered. Over the last month I’ve been included in an email group comprising over 250 practicing physicians from all over the world sharing their knowledge and experience. Three members of that group are here today.
To me it is obvious that we should robustly explore every possible treatment to combat this pandemic at every stage of the disease. Why has there been such resistance to low-cost, off-the-shelf therapies that might stop the progression of Covid 19 and help keep people out of hospitals and the intensive care units? I hope today’s hearing can answer that question and provide direction on how to correct this glaring blunder that has cost far too many lives....
Ends at 7:01
Beginning at 14:58:
Our first witness is Dr Peter McCullough. Dr McCullough is the current Vice Chair of Internal Medicine at Baylor University Medical Center and a Professor of Medicine at Texas A&M College of Medicine. Dr McCullough received his MD from the University of Texas Southwestern Medical School and his MPH from the University of Michigan. Dr McCullough is Board Certified by the American Board of Internal Medicine in the areas of internal medicine and cardiovascular disease. He specializes in the treatment of patients with complicated internal medical problems that has affected major affected major organs including the heart and kidneys. Dr McCullough.
Dr. Peter McCullough: Thank you Chairman Johnson, ranking member Peters and members of the committee for allowing me to talk to you today about the critical need for early ambulatory treatment for covid19 as an emergency measure in the middle of this national crisis....
Ends at 15:49
Beginning at 16:42:
My viewpoint is this pandemic should have always been viewed as having four pillars. If we can bring up the figure.
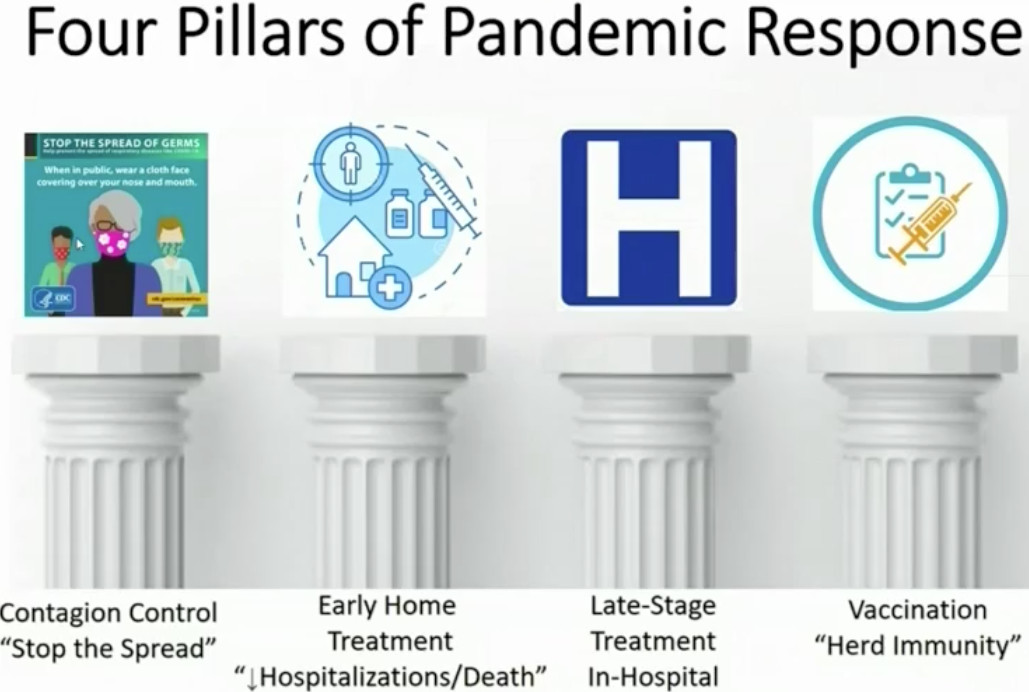
The first pillar is contagion control. We have had probably the vast majority of government efforts solely focused on contagion control. The entire media representation of what the government has been doing has been on contagion control. As we see it here today, it’s obvious contagion control has not solved the problem. The second pillar is early ambulatory treatment. This virus infects individuals and they sit at home for two weeks. We have a two-week opportunity to treat this problem and we hear nothing about it. We hear nothing about early ambulatory treatment. There’s no updates. There’s no viewpoint to Americans of what’s going on outside of the United States where early ambulatory treatment is a standard of care in countries that are doing much better than the United States. It’s grossly overlooked....
Ends at 17:36
snapshot taken on 5 December 2020
Countries based on current HCQ/CQ usage

COVID-19 Treatment - Analysis of 192 global studies showing high efficacy for early treatment
COVID-19 studies for: HCQ - Ivermectin - Vitamin D - Zinc - REGN-COV2 - LY-CoV - Remdesivir
With this pandemic and this virus what we’ve learned is that there’s an early viral replication phase followed by a destructive immune activation called cytokine storm and then blood clotting thrombosis.
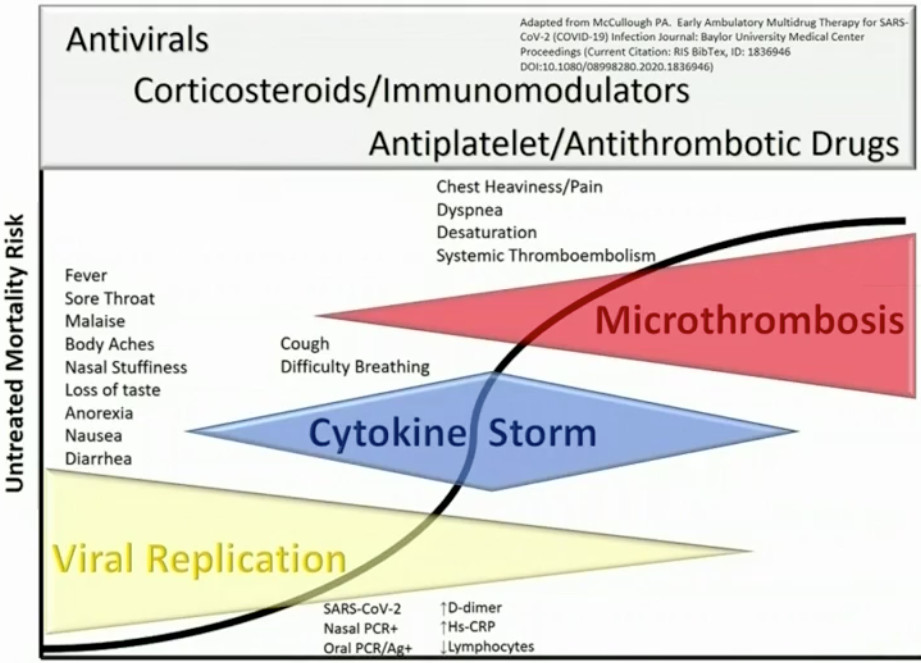
What doctors have done is they’ve innovated and they’ve identified, both in the hospital and outside of the hospital, aided by clinical trials and observational studies, an approach that involves combination antivirals, followed by corticosteroids and antithrombotic agents. Doctors in the outpatient communities, faced with thousands of patients calling and begging for help, have innovated. Dr Zelenko is one in New York, in the middle of the calamity in New York, who was an early innovator.
I summarized these and published them in the American Journal of Medicine, the synthesis of the principles of randomized trials and observational studies and this algorithm has been updated multiple times. It provides a framework for new drugs and agents to be incorporated in an early inventory treatment approach.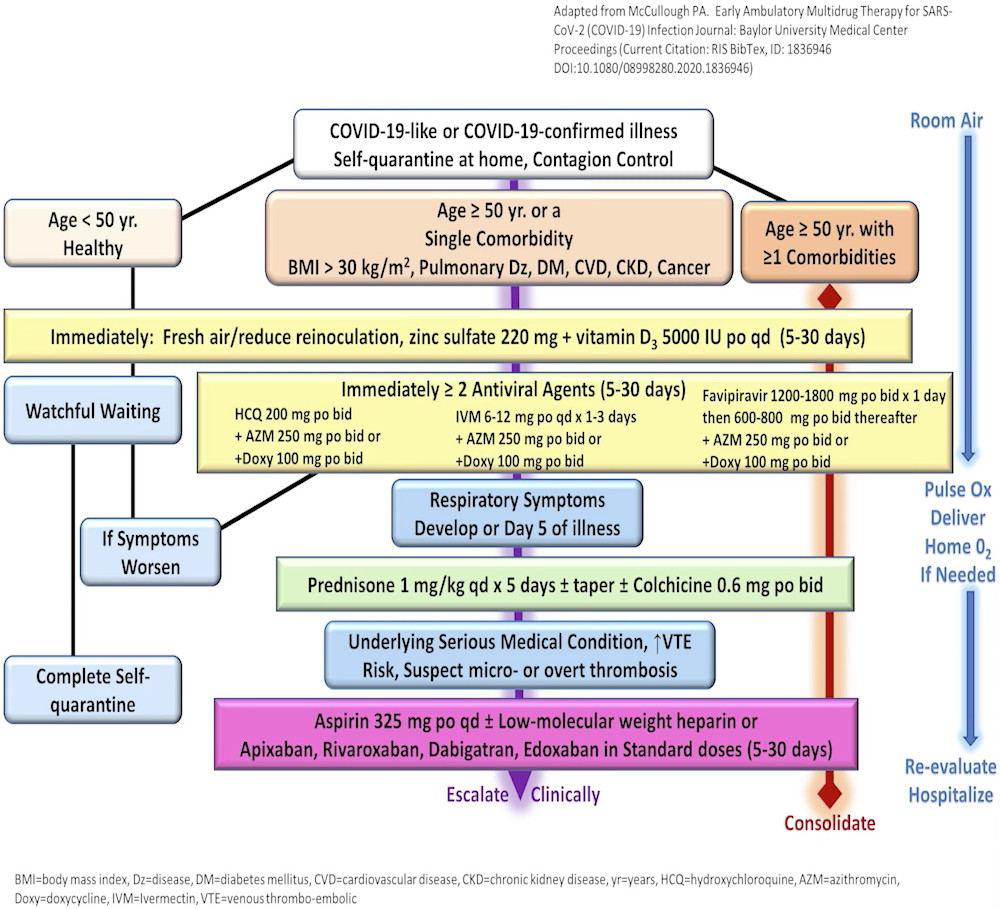
I’ve reviewed every report from real world data from American doctors who have innovated and faced this problem and I can tell you that they are achieving rates of hospitalization and death less than three percent for high risk Americans over fifty with multiple conditions. Most doctors can achieve less than one percent. With no treatment in the United States right now, an individual over fifty with medical problems faces a seven percent rate of hospitalization and death. Someone in their 80s, that skyrockets to 40 percent.
I can tell you as a doctor I have always treated high risk patients with the best tools available and I looked at all the evidence. When it was obvious that AIDs drugs didn’t work I didn’t use them. But hydroxychloroquine, ivermectin, if I had favipiravir, I’d combine it with other drugs, and then steroids. That should be non-controversial. Doctors should be using corticosteroids in patients and outpatients—they’re supported by both inpatient and outpatient studies—as well as blood thinners. What doctor would not help a patient who’s at risk for a catastrophic stroke that occurs as a complication of this condition?
So I can tell you right now I’m not asking for permission to do this but I’m asking for your help. I’m asking for the government to organize all government agencies that are related to this to assist doctors rapidly with their innovation and their compassionate care of patients with Covid 19 at home because we can prevent hospitalization and death and right now it’s the only option on the table. Thank you....
Ends at 20:50
Beginning at 45:29:
Senator Johnson:
Obviously we have a huge disconnect between testimony here, between experts, Harvard and Yale educated doctors and PhDs.
Dr McCullough, I know the 93% increase in poison reporting sounds pretty scary. You’d mentioned before the hearing a little bit about what that’s based on. Can you can you talk about that? And also you’ve had Covid. You’ve recovered from it. Not totally. You’re tested negative so you don’t represent a danger. But can you first of all talk about that 93% increase in safety or in poison reportings and then also just talk about your own personal experience with your own treatment?
Dr McCullough: Senator I want my testimony to clearly recognize—be on the record that I think Dr Jha’s testimony is reckless and dangerous for the nation and his comment regarding the poison control reporting is exactly what Dr Peters is interested in. You’re interested in misinformation regarding covid.
That report in the middle of the pandemic, when hydroxychloroquine early on was appropriately used, that first wave of the pandemic—that’s what kept it from rocketing, skyrocketing. Hydroxychloroquine was widely used early on. That’s what kept the March-April-May curve down. Okay?
When it was used—and we had 500,000 dose administrations of hydroxychloroquine, the Poison Control Center received, I think the number was, 77 additional calls. And when the reviewer looked at it, [for] two-thirds of them, somebody took an extra dose and they were concerned. So it boiled down to 17 cases out of over 500,000 administrations. And yet Dr Jha holds that up to the American public as a scare point, to scare the public away from a safe and effective therapy for Covid 19.
And as you mentioned I had it myself. I’m 57. I’ve got asthma, I’ve got atherosclerotic cardiovascular disease. I can tell you Senator Peters, I was not falsely reassured sitting at home. Believe me, when I got that test result I was terrified. And every American is terrified. Every older patient with heart and lung disease, when they get the report, they’re not falsely reassured and sit at home, think this is going to be a picnic. They are scared to death and by the time they come to the hospital it is frank terror because they know they’re going to be isolated, they’ll never see their family members again.
What did I do? I did the right thing. I got myself rapidly into a FDA approved treatment protocol through a study. Hard to do by the way because the government offers no resources to the public to quickly get into clinical trials. I got into a clinical trial. I took hydroxychloroquine as part of a multi-drug sequence program which is exactly what’s in the peer-reviewed literature which is the framework of how Americans should be treated.I was a few days behind in recognizing what was going on. The virus got into my lungs. I had pulmonary involvement and I got anxious. I got to the point where I thought maybe I could be hospitalized and I can tell you firsthand this cocktail of drugs works for sure but hydroxychloroquine dose by dose, settles down that fever, settles down, reduces the amount of the severity, intensity of symptoms and by that mechanism that’s the reason why hydroxychloroquine reduces hospitalizations and death.
When patients get anxious and they can’t breathe anymore they go to the hospital. So this isn’t complicated. There’s over a hundred studies. They are all supportive. The EUA says when the preponderance of evidence shows the drug works and has acceptable safety we ought to go. My view is we need to go with this on everybody high risk in America....
Ends at 49:17
correlates meta analysis of an increasing number of studies
snapshot taken on 5 December 2020
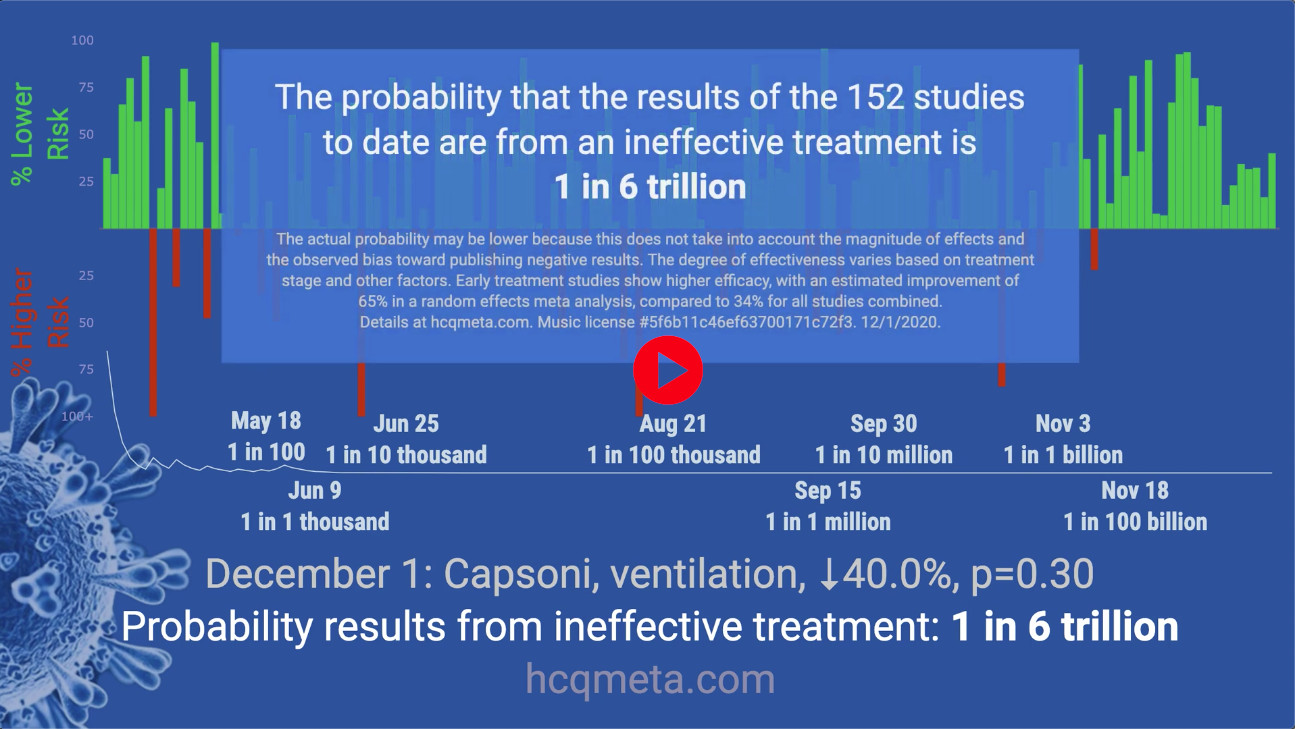
HCQ is effective for COVID-19 when used early: meta analysis of 156 studies
Version 28, December 4, 2020
Beginning at 1:49:57:
Senator Johnson: What didn’t necessarily have to take time was using off-the-shelf drugs for early treatment. But yet somehow, I guess it’s because President Trump allowed the word hydroxychloroquine to flow off his, you know, out of his mouth, all of a sudden that was attacked and that was poisoned and we never ever had the NIH, CDC, FDA put their full weight behind an investigation of that—the full clinical trials—I was pushing, I was pushing for that. Not pushing hydroxychloroquine. Pushing for the science, for studies. But it never happened because, again, it was censored. We talk about disinformation. Not providing the public information is disinformation as well.
So again why I fault the agencies is because they they turned a blind eye toward simple, cheap, possibly effective treatments that by the way created no harm. Dr Risch, I think you mentioned and I’ve got a lot to go over here, you mentioned that the non-randomized trials, I guess we’d call that observational studies, real world experience, really involving thousands of patients, indicated that there was a 50% reduction in hospitalization deaths. In the Saudi Arabian study, five time reduction. Now let’s let’s just assume that that’s true. I think we can also take a look at the billions of doses a year that are prescribed of hydroxychloroquine. Any member of Congress has gone to Africa, they’ve just been handed hydroxychloroquine as an anti-malarial. We treat lupus, we treat rheumatoid arthritis. We don’t give EKGs before that.
The studies I saw early on were designed to fail on hydroxychloroquine, late in treatment when people are basically ready to die or when their heart was already affected by the virus. Of course hydroxychloroquine does have an impact on arrhythmia at that late stage but not early which is when it was being recommended—for early use, first five days. So when you take a look at the risk-reward, now that these other observational non-randomized trials have been—or studies have been—conducted, 50% or five-fold reduction in death and hospitalization versus the almost infinitesimal risk of hydroxychloroquine and zinc? This has made no sense to me what so ever. The only explanation is the politicization of it which I opened up my opening comments saying that has been what’s such a shame.
I do want to—before I forget—I received a letter and an article from the Economic Standards submitted by Dr Stephen Hatfield. The letter kind of explains what I have known about a whistleblower, Dr Rick Bright, who was asked by his superiors to work on establishing a FDA expanded access investigational new drug protocol. But by his insubordination, he instead went to Janet Woodcock and people in the FDA and got the Emergency Use Authorization. Which sounds like, Hey we’re going to expand the use of this. No, he dramatically restricted the use of hydroxychloroquine—only in hospital. What I think we all recognize is probably not particularly effective, possibly dangerous and only out of the national stockpile. He knew what he was doing. That’s what poisoned the well. That’s what created what I’ve called the prescription log jam here on hydroxychloroquine or early—and I think it affected all early treatment options. It took them off the table. We took our eye off the ball. That’s why I say our agencies failed us. These individuals in these agencies failed us.
And here’s the question I want to ask for you Dr McCullough because you mentioned this. The circle of empathy. Can you just talk about how you described that to me before the hearing?
Dr McCullough: Let me just say before I answer that that this is not just a government culpability and malfeasance with respect to hydroxychloroquine. This is academic malfeasance. There were two fraudulent papers, one in the New England Journal of Medicine [18 June 2020], one in Lancet [22 May 2020], published by individuals interested in doing evil to the world with respect to a beneficial treatment of hydroxychloroquine. In an unprecedented manner these two manuscripts were withdrawn after two weeks where they could scare the public and the world’s physician audience. Since that time there have been dozens of fraudulent papers—
Senator Johnson: Re-emphasize that. They were then withdrawn.
Dr McCullough: They were withdrawn and the New England Journal of Medicine and Lancet acknowledged that they were fraudulent papers. They were scare papers, to scare people on hydroxychloroquine. Since that time there’s been dozens of pile-on scare tactics in academics. This isn’t the government. This is people in my field, in academic medicine who are committing academic fraud.-
[See analysis:
- Lancetgate: why was this “monumental fraud” not a huge scandal?, Daniel Espinosa, Dissident Voice, 20 Aug 2020
- The Media Sabotage of Hydroxychloroquine Use for COVID-19: Doctors Worldwide Protest the Disaster - Media and Big Pharma are in lockstep to suppress a cheap, life-saving Covid-19 therapy in order to reap pandemic-sized profits, Elizabeth Woodworth, Global Research, 30 Jun 2020
I reviewed a paper—I’m a cardiologist—I reviewed a paper that made it into the medical literature demonstrating that hydroxychloroquine causes a heart attack, that hydroxychloroquine causes a giant scar in the heart. And I can tell you, I’m at Baylor in Dallas, we have the world’s most recognized Cardiac Pathology Program in the world. Our Senior Examiner has held in his hands more human hearts than anybody in the history of mankind. I can tell you firsthand hydroxychloroquine does not cause giant scars in the heart.
So academic medicine is committing a fraud, is committing, I think, a crime against humanity. There must be a motivation behind this that’s much bigger than just democrat versus republican. I am extremely concerned, honestly, about the the academic contribution to scare tactics in the world. Now it’s not working everywhere. In India it’s given first line and India is such a crowded country. I’ve been there myself. Their deaths per million population is a tiny fraction of America.
Senator Johnson: Isn’t it 95 versus over 700?
Dr. McCullough: Yeah.
Senator Johnson: And they’re using hydroxychloroquine.
Dr McCullough: Right. We have nearly 800 deaths per million population in the United States and we’re all spread out. In India, they’re on top of each other, they have less than 100 deaths per million population. The leading doctor in India is willing to come testify to the United States and tell you the reason why. They have tons of Covid. It’s spreading over like crazy. But they’re treating it at home with hydroxychloroquine and other drugs. Remember, it’s a multi-drug program probably about four or so drugs plus supplements and they’ve handled the infection.
Greece. Everyone’s traveled in Europe. Greece is not a third world country. First line, you’re given hydroxychloroquine Okay? We’ve missed the ball. There’s 30 countries that have approved an oral version of remdesivir here called favipiravir—30 countries including Japan!
Every country that is actually having a reasonable public health response is treating this problem at home. Now none of these drugs are a cure. But they allow the patient to get through the illness like myself. I missed 10 days off of work and I returned to the workforce. I didn’t get in the hospital for four weeks. They allow people to stay at home and not go out and contaminate other people. My wife and I got it at the same time and because we were treated at home we were actually able to stay at home so we didn’t contaminate other people.
The current program—that’s supported by the minority witness and the National Institutes of Health and all government bodies—is that patients go home, they get no help whatsoever, doctors are not supposed to treat them, they go out in a panic to Urgent Cares and ERs, contaminate more people and then they’re hospitalized and die. America has to wake up right here right now. We are getting buried and we need home treatment.
Ends at 1:58:06
Beginning at 2:04:40:
Dr Ashish Jha:
It’s always possible that any one of us can be wrong. At that point I look to consensus opinion among experts. I’ll go—for instance on infectious disease issues like this—I will go to the Infectious Disease Society of America because they are made up of our leading infectious disease experts. IDSA does not recommend the use of hydroxychloroquine for outpatient therapy for Covid 19 and they recommend against it for inpatient therapy. I will turn to agencies like the National Academy of Medicine. I will turn to the National Institutes for Health. I will listen to people like Dr Francis Collins.
The point is that the idea is that these are all individuals with incredible expertise looking at the data. So could it be that I am wrong and Dr Risch is right. Well sure, people can disagree. But when you look at the broad consensus in the American scientific community, basically the scientific consensus is very clear that hydroxychloroquine is not effective. Now when we have looked at in the outpatient setting, and I started with this in my testimony, we don’t have great data on the outpatient setting. We have a small number of studies. But the best one above those show that it doesn’t work. Could we get better data? Absolutely. And so Senator, I would love it if you would push for better quality randomizing—
Senator Johnson: By the way, I have, I have and they wouldn’t do it. Okay? I’ve had a direct pipeline to Dr Hahn and I cannot get them to do it. Which again begs the question, Why not? That’s why I say this has been an enormous dereliction and again what I would say, you can maybe turn to those different places but as a patient, myself, I wanted to get hydroxychloroquine and I couldn’t get it. Okay? I think I should have the right to try—in dealing with my doctor who I trust—who I trust, I’m sorry more than some of these people who are so outside the circle of empathy and for whatever reason. Again I’m sorry, it’s just me, I question the fact that because this cocktail costs about 20 bucks and remdesivir costs 3,000, that maybe there’s a little bias, maybe there’s a little conflict, maybe there’s a little agenda that’s outside of really what’s treating a patient; when you’re in the ivory tower and you’re not dealing with sick and dying and ventilated patients.
So now I want to talk about remdesivir, the three of you here. Talk about what the study was on remdesivir. How strong a science that is and what kind of dangerous side effects remdesivir causes? And yet, that’s that’s the drug that’s been pushed. That’s the one that got the Emergency Use Authorization. So whichever one of you feel you’re most qualified to talk about remdesivir.
Dr McCullough: I’ll just make a few comments to just say that with any one of these randomized trials, even remdesivir, in my view, my judgment of the evidence is that they’re all inconclusive. So if you look at remdesivir in many of the inpatient studies—Do you know what the end point that they use? They actually use an endpoint that the physician decides. The physician decides how much oxygen the patient needs and if the patient changes in a grade of oxygen they change on an ordinal scale.
The entire randomized biopharmaceutical complex right now is basically corrupt. The data on remdesivir are mixed. But I just had a patient die last week, received remdesivir. The difficulty is it’s too toxic. It causes liver toxicity. He had liver toxicity, can’t get through the five dose administration, and the drug is administered too late. The problem is the virus was replicating two weeks ago. By the time he got into the hospital the virus has already done its job. So it’s a fool’s errand to test a single drug like remdesivir late in the illness. This is no different than HIV. We need multiple drugs early up front and the best we have right now are these mixes of vitamin supplements and then the generic medications—the best we have.
Now, listen the NIH just has some oral drugs that they’re sponsoring with pharmaceutical trials to move forward. If there’s an oral drug tomorrow that can fit into a treatment protocol it’s ready to go. We can we can plug it right in. The NIH and biopharmaceuticals right now have delivered zero oral medications to doctors in practice. Zero. That’s our batting average right now. So for all the science we’ve put into this, as a country with the greatest pharmaceutical companies in the world, zero oral drugs for the next patient who gets sick with Covid 19.
Senator Johnson: Isn’t it also true that in the study that was being conducted on remdesivir, very late in the trial because it was showing no improvement in terms of reducing deaths but it was showing an improvement in terms of reduction number hospital days, that they actually switched the outcome that they’re going to judge?
Dr McCullough: Okay, there’s so many flaws to the clinical trials that people are looking to. One of the rules is we never change the primary endpoint. The second rule is we have an objective endpoint. The number of days someone stays in the hospital is not objective. That’s determined by whether or not the patient feels like they’re ready to go home, where the doctor discharges them, social delays and everything else. So none of these trials—none of the trials—minority witness says he wants to use the word evidence, evidence, evidence.
Listen, we’re in a crisis. We need both the art and the science of medicine. What these doctors are telling you and what the real world evidence is telling you is that patients using the sequence multi-drug approach, at home, is the only chance to reduce hospitalization. Remdesivir doesn’t prevent a hospitalization because you have to be in the hospital to get it.
Senator Johnson: One thing I completely agree with Dr Jha is the workforce issue. The doctors I’m talking to in Wisconsin say that our hospitals currently aren’t being overwhelmed, but they may based on the uptick of the surge in cases. But the biggest problem they have in hospitals is they don’t have the workforce. Which again speaks to had we really put and focused on early treatment and prophylaxis you might have a more ready workforce. But you’ve got—nurses and doctors have to stay home because schools are closing, they got to take care of their kids. Again, we have not, from my standpoint, done a very good job of really addressing this in a logical way. Just talking, It’s got to be testing. And now It’s got to be vaccine. But we are we are missing, to me, the key ingredient to solving this crisis which is early effective treatment. We ought to be pouring billions of dollars, but because of the scare tax on hydroxychloroquine—I know because I talked about why haven’t we done the studies? Because we scared people away from participating in the trials in the U.S. They tried to do a study and they couldn’t get people participating.
Dr Risch, can you talk again [about] the difference between a random controlled trial and a non-random or just observational studies or just real world experience and the validity of all.
Dr Harvey Risch: Let me start with the last point, real world experience. After I had published my paper in the American Journal of Epidemiology in May [Harvey A Risch, Early Outpatient Treatment of Symptomatic, High-Risk COVID-19 Patients That Should Be Ramped Up Immediately as Key to the Pandemic Crisis, American Journal of Epidemiology, Volume 189, Issue 11, November 2020, Pages 1218-1226, https://doi.org/10.1093/aje/kwaa093, Published 27 May 2020] I got emails from a number of clinicians across the country saying that they had been using hydroxychloroquine very effectively. Now the criticism of that is those people cherry-picked themselves to tell me that they were doing well and all the people who weren’t doing well didn’t report it and they didn’t tell me. So I said to two of them, Okay why don’t you go back, keep doing what you’re doing and I’ll follow up with with you in a month or six weeks and see how you’ve done after that. So we’re no longer cherry picking. We’re setting them as test candidates for their treatment plans.
After about six weeks I went back. This was Dr Zelenko in New York and Dr Procter in Texas. And after six weeks what I found is Dr Zelenko had treated another 400 patients and had no deaths, in those—another 400 high-risk patients. He has treated 3,000 patients now but those were 400 patients since the first time that I talked to him and no deaths. Dr Procter had at that time about 180 patients subsequent to when I first talked to him again and I think he had one death in that.
So their real world evidence is such that no rational person would say I’m not going to go to them. If I get sick, they’ll be the first person that I would go to because they’ve already proved that they can do this. Whatever it is they’re doing, their magic, whatever their treatment recipes are, it’s working and they’re saving their patients.
Senator Johnson: Just real quick. You said there was one death. Death from covid. Not from hydroxychloroquine.
Dr Risch: It was actually, it’s not even clear that it was a death from Covid. The person had a heart attack out of the blue that was unrelated. It was two weeks past. They had finished all the treatment and so he wasn’t even sure whether it was related to Covid. But he put it there to be conservative. He put it in, but it’s so it’s not even clear. It was an elderly man.
That’s the first thing. The second part about real world evidence and non-randomized trials is the only benefit of a randomized trial is if there are some unknown variables that you can’t control for. All the known things that you can measure on people you can adjust for in your study, you can match on in the study and you can remove them for bias so that you can have a pure treatment between the people who take the drug and the people who don’t. It’s only the unknown variables and the reason why these non-randomized but controlled studies have converged to randomized ones is we’ve learned enough about the diseases that we study that we know what else to measure by and large in every one of them. So we measure everything in the world and we control for them and that has removed the so-called unknowns of bias. And this is why there’s a difference in non-randomized trials now compared to in the 1950s when we didn’t know enough about what to measure and how to control for it. So that’s the second issue, that empirically we know that non-randomized but well-controlled trials work just as well as randomized ones.
Ends at 2:14:55
Beginning at 2:20:27:
Dr McCullough: I’m in close communication for this worldwide disaster with many countries and I can tell you I did a program with Eamonn Mathieson at the Covid Medical Network in Australia to show you how off-kilter the world is. [Webinars: EARLY COVID TREATMENTS: Guest Speaker - Prof Peter McCullough MD, Presented by Dr Eamonn Mathieson, Anesthetist, Covid Medical Network, Convenor. 14 Nov 2020 (32:46)] In Queensland, Australia a doctor will be put in jail for prescribing hydroxychloroquine. If you go over to India they’re going to give it to you right away. In Greece they’re going to give it to you right—it’s in their guidelines.
Senator Johnson: It’s over-the-counter in some countries.
Dr McCullough: Yeah. But my point is we’re all the way from: They give it first line, in their guidelines, the Greek guidelines give hydroxychloroquine but in Queensland you get put in jail. In the United States we’re caught up in this flurry of data and confusion. Something is going very wrong in this world.
Senator Johnson: I was contacted by a doctor who I think had written four prescriptions for hydroxychloroquine. Four. And she was issued a grand jury subpoena by the Homeland Security Investigation Department, if you can believe that. A doctor prescribing an approved drug and she gets a grand jury subpoena. Something’s not right about that, okay? Now because I checked into it they withdrew that subpoena but there’s there’s something that has gone wrong here. There’s something that is not right and I for one intend to get to the bottom of it....
Ends at 2:21:52