This is a partial annotated transcript of Dr Pierre Kory testifying on 8 Dec 2020 before the Senate Homeland Security Committee Hearing on Medical Response to COVID-19. Source of this recording: https://www.c-span.org/video/?507035-1/medical-response-covid-19
Pierre Kory, MPA, MD is a founding member and President of the Front Line COVID-19 Critical Care (FLCCC) Alliance and co-author of the MATH+ and I-MASK+ Prophylaxis and Treatment Protocols for COVID-19. Dr Kory is the former Chief of the Critical Care Service and Medical Director of the Trauma and Life Support Center at the University of Wisconsin. He is considered one of the world pioneers in the use of ultrasound by physicians in the diagnosis and treatment of critically ill patients. He helped develop and run the first national courses in Critical Care Ultrasonography in the U.S., and served as a Director of these courses with the American College of Chest Physicians for several years. He is also the senior editor of the most popular textbook in the field titled “Point of Care Ultrasound,” a book that is now in its 2nd edition and that has been translated into 7 languages worldwide. He has led over 100 courses nationally and internationally teaching physicians this now-standard skill in his specialty.
Dr Kory was also one of the pioneers in the United States in the research, development, and teaching of performing therapeutic hypothermia to treat post-cardiac arrest patients. In 2005, his hospital was the first in New York City to begin regularly treating patients with therapeutic hypothermia. He then served as an expert panel member for New York City’s Project Hypothermia, a collaborative project between the Fire Department of New York and Emergency Medical Services that created cooling protocols within a network of 44 regional hospitals along with a triage and transport system that directed patients to centers of excellence in hypothermia treatment, of which his hospital was one of the first.
In collaboration with Dr Paul Marik, Dr Kory pioneered the research and treatment of septic shock patients with high doses of intravenous ascorbic acid. His work was the first to identify the critical relationship between the time of initiation of therapy and survival in septic shock patients, an aspect of the therapy that led to understanding all the failed randomized controlled trials that employed delayed therapy.
Dr Kory has led ICU’s in multiple COVID-19 hotspots throughout the pandemic, having led his old ICU in New York City during their initial surge in May for 5 straight weeks, he then travelled to other COVID-19 hotspots to run COVID ICU’s in Greenville, South Carolina and Milwaukee, Wl during their surges. He has co-authored 5 influential papers on COVID-19 with the most impactful being a paper that was the first to support the diagnosis of early COVID-19 respiratory disease as an organizing pneumonia, thus explaining the critical response of the disease to corticosteroids.
The Senate Homeland Security and Governmental Affairs Committee heard from medical professionals who advocate for alternative COVID-19 treatments and mitigation measures to those of the National Institutes of Health, Centers for Disease Control and Prevention, and World Health Organization. Several of the doctors advocated for the use of the drugs hydroxychloroquine and ivermectin to treat patients and questioned the efficacy of masks, social distancing, and quarantining. After Ranking Member Gary Peters (D-MI) delivered his opening statement criticizing the hearing, no Democrats participated in the proceeding.
Beginning at 0:15:00:
Senator Johnson:
Good morning. This hearing is called to order. Let me start by thanking our witnesses, first and foremost, for being doctors. I just have the greatest respect for anybody that has dedicated their lives to saving other people's lives and improving the health of their patients, and focusing first and foremost on their patients. So i really want to thank you for that. i want to thank you for taking the time to prepare testimony and appear before us in person and via webex.
In his reflections on Progress Peaceful Coexistence and Intellectual Freedom, Russian Dissident Andre Sakarov wrote:
The second basic thesis is that intellectual freedom is essential to human society—freedom to obtain and distribute information, freedom for open-minded and unfearing debate, and freedom from pressure by officialdom and prejudices. Such a trinity of freedom of thought is the only guarantee against an infection of people by mass myths, which, in the hands of treacherous hypocrites and demagogues, can be transformed into bloody dictatorship. Freedom of thought is the only guarantee of the feasibility of a scientific democratic approach to politics, economy, and culture.
In today's biased news media and social media, within academic journals, on college campuses, in government agencies, in ivory towers, we are losing the freedom to obtain and distribute information. The reaction to our first hearing on Early Treatment is but one example. Although not surprising in today's hyperpartisan climate, it is still shocking. In that hearing we heard from Dr. McCullough, a cardiologist and Vice Chair of Medicine at Baylor University Medical Center, Dr. Harvey Risch, Senior Professor of Epidemiology at Yale University and Dr. George Fareed, trained at Harvard University and the National Institutes of Health. Combined, these Doctors have more than 900 scientific research publications, extensive drug development experience, more than 80 years clinical practice, including treating more than 1,000 high-risk Covid patients along with thousands of other lower risk Covid patients.
I was hoping that, post-election, by asking such eminently qualified Doctors to testify about the rationale for and growing effectiveness of early treatment minds could be opened and lives could be saved. Unfortunately the Democrat witness Dr. Ashish Jha began tweeting his negative viewpoint of early treatment before the hearing even began and continues his media blitz for days afterward. Most obnoxiously, and it was obnoxious, he penned an op-ed that the New York Times ran and headlined, “The Snake Oil Salesman of The Senate”. The absurdity of calling Dr. Jha as a witness or paying any attention to him in the media was demonstrated when i asked him during the hearing, Have you treated any Covid patients? His reply, I have not, sir.
Dr. McCullough also talked about The Circle of Empathy in Medicine. Those who actually treat Covid patients are in the center. Not only have they shown extraordinary courage, exposing themselves to the disease, they also have the greatest empathy for patients who experience the fear and loneliness of a Covid diagnosis. These are the medical practitioners, the heroes, that experts in the ivory towers in media have chosen to ignore and vilify. The experts far outside The Circle of Empathy had developed in support of the current NIH guideline of providing no treatment at all until patients are sick enough to require hospitalizations. As we are all aware, at that point, treatment is often too late.
So here we are again, holding a second hearing to obtain and distribute information on what is known about early treatment of Covid. What could possibly be controversial about that? Yet some are calling this hearing dangerous, and instead of waiting until after the hearing to trash this information and our witnesses the New York Times and other publications have already run preemptive attacks, implying this hearing is anti-vaccine. So let me be clear. This hearing like the first hearing is focused on Early Treatment of Covid. It is not about vaccines. End of story. In my opinion, discouraging and in some cases prohibiting the research and use of drugs that have been safely used for decades has caused tens if not hundreds of thousands of people their lives. By the time any vaccine is fully deployed, no matter how successful, how effective, how safe, millions more will become infected. With effective early treatment fewer people will get seriously ill, and fewer people will die. So why not give early treatment a shot? What have we got to lose?
And finally, Why is there such a concerted effort to silence the voices of courageous health professionals promoting early treatment? It makes no sense. Let me make just a final point. At the beginning of this epidemic, when I first heard about the potential of hydroxychloroquine, it intrigued me because, to me, a drug like that, that's been around for 65 years, shown to be safe, it's cheap. Billions of tablets are produced every year. We could have ramped up production. If that could be proven to be effective, wouldn't that be the dream solution? Why didn't we pursue that, and ivermectin and favipiravir. Why didn't we look at these drugs that were already there, generic, cheap, mass producible? Again, it makes no sense....
Beginning at 0:28:05:
Senator Johnson:
Our next witness is here in person, Dr Pierre Kory. Dr Kory is the former Associate Professor and Chief of the Critical Care Service and Medical Director of the Trauma and Life Support Center at University of Wisconsin and recently joined the ICU Service at Aurora St. Luke Medical center in Milwaukee. He is Board Certified in Critical Medicine, Pulmonary Diseases, and Internal Medicine. Dr Kory has traveled across multiple states in the U.S. to care for COVID-19 patients throughout the pandemic. He is also the President of The Frontline COVID-19 Critical Care Alliance, a nonprofit organization of critical care specialists led by Professor Paul Marik, whose mission over the last nine months has focused on the research and development of effective treatment protocols for COVID-19 using repurposed drugs. He received his MD from St. George’s University School of Medicine. And I’ll only add that we added Dr Kory very late to a hearing in May, because I had heard of his development of, I guess, anti-inflammatory steroids in critical care on COVID. And Dr Kory I have to tell you I’ve had Doctors come up to me and thank me for holding that hearing where they listened to you, changed their thinking, they believed they’ve saved their patient’s lives because of your testimony at that hearing. I hope your testimony will be as impactful today. Dr Kory.
Pierre Kory, MD: Senator, thank you, and thank you for holding this hearing. I just want to start out—I didn’t think I’d have to say this—but I want to register my offense at the Ranking Member’s Opening Statement. I was discredited as a politician. I am a physician and a man of science. I have done nothing, nothing but commit myself to scientific truth and the care of patients. And to hear that I’m here because of a political angle, I am not a politician, I’m a physician.
I want to start out by saying that I’m not speaking as an individual. I’m speaking on behalf of the organization that I am a part of. We are a group of some of the most highly published physicians in the world. We have near 2,000 peer reviewed publications among us. Led by Professor Paul Marik, our intellectual leader, we came together early on in the pandemic and all we have sought is to review the world’s literature on every facet of this disease trying to develop effective protocols.
You just mentioned that I was here in May and I touted—I wouldn’t say touted—I recommended that it was critical that we use corticosteroids in this disease when all of the national and international health care organizations said we cannot use those. That turned out to be a life-saving recommendation.
I am here again today with a new recommendation. In the last nine months in our review of all of the literature as a group—again we are some of the most highly published physicians in our specialty and the world—we have done nothing but try to figure out how to identify a repurposed and available drug to treat this illness. We have now come to the conclusion, after nine months—and I have to point out, I am severely troubled by the fact that the NIH, the FDA and the CDC, I do not know of any task force that was assigned or compiled to review repurposed drugs in an attempt to treat this disease. Everything has been about novel and/or expensive pharmaceutically engineered drugs, things like tocilizumab and remdesivir and monoclonal antibodies in vaccines.
We have [one] hundred years of medicine development. We know, we are expert in all the medicines we use, and I do not know of a task force that has been focused on repurposed drugs. I will tell you that my group and our organization, I will say that we have filled that void. That is all we have done, is focused on the things we know and things we do.
I’m here to tell you, Dr Rajter, he just presented. He has one study of the many that I want to talk about. I want to talk about that. We have a solution to this crisis. There is a drug that is proving to be of miraculous impact. And when I say miracle, I do not use that term lightly. And I don’t want to be sensationalized when I say that. That is a scientific recommendation based on mountains of data that has emerged in the last three months.
When I am told, and I just heard this in the opening sentence, that we are touting things that are not FDA or NIH recommended, let me be clear: the NIH, their recommendation on ivermectin, which is to not use it outside of controlled trials, is from August 27th. We are now in December. This is three to four months later. Mountains of data have emerged from many centers and countries around the world showing the miraculous effectiveness of ivermectin. It basically obliterates transmission of this virus. If you take it you will not get sick.
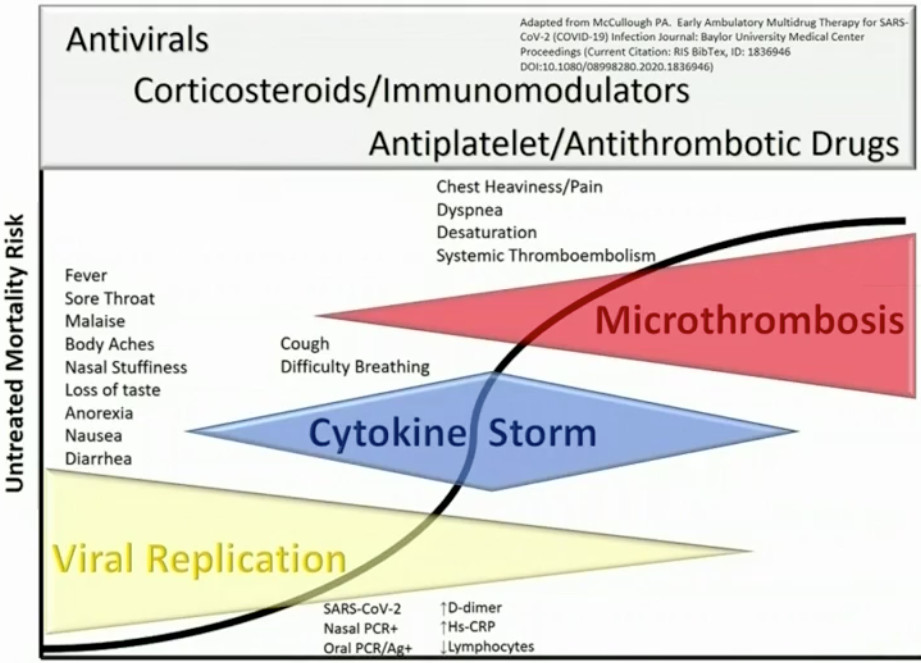
I want to briefly summarize the data. My manuscript, again published by some of the most—we have contributed more to the medical knowledge of our specialty in our careers than anyone else can claim as a group. Our manuscript which was posted on medicine preprints server details all of this evidence. [Review of the Emerging Evidence Demonstrating the Efficacy of Ivermectin in the Prophylaxis and Treatment of COVID-19, FLCCC Alliance; updated Jan 12, 2021]
I want to briefly summarize it.
Number One: We have evidence that ivermectin is effective, not only in prophylaxis, in the prevention. If you take it you will not get sick. We just came across a trial last night from Argentina, by the lead investigator of ivermectin in Argentina, Dr Hector Carvallo. They prophylaxed 800 healthcare workers. Not one got sick. In the 400 that they didn’t prophylax with ivermectin, 58% got sick. 237 of those 400 got sick. If you take it you will not get sick. It has immense and potent antiviral activity.
We know that from the first study of Monash [Caly, L., Druce, J.D., et al. The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro, Antiviral Research, Volume 178, 2020, 104787, ISSN 0166-3542, doi.org/10.1016/j.antiviral.2020.104787], it has made the bench to the bed side. Prophylaxis: we now have four, large randomized control trials totaling over 1,500 patients, each trial showing that as a prophylaxis agent it is immensely effective. You will not get sick. You will be protected from getting ill if you take it.
In early outpatient treatment we have three randomized control trials and multiple observation as well as case series showing that if you take ivermectin the need for hospitalization and death will decrease.
The most profound evidence we have is in the hospitalized patients. We have four randomized control trials there, multiple observation trials, all showing showing the same thing: you will not die or you will die at much much much lower rates statistically significant large magnitude results if you take ivermectin.
It is proving to be a wonder drug. It already won the Nobel Prize in Medicine in 2015 for its impacts on global health in the eradication of parasitic diseases. It is proving to be an immensely powerful antiviral and anti-inflammatory agent. It is critical for its use in this disease.
We again, stand by our manuscript, it is a scientific manuscript. It’s been submitted for peer review. But please recognize, peer review takes time. It takes months. We do not have months. We have 100,000 patients in the hospital right now dying. I’m a lung specialist. I’m an ICU specialist. I’ve cared for more dying Covid patients than anyone can imagine. They’re dying because they can’t breath. They can’t breath. They’re on high-level oxygen delivery devices, they’re on non-invasive ventilators and/or they’re sedated and paralyzed and attached to mechanical ventilators that breath for them. And I watch them every day. They die. By the time they get to me in the ICU they’re already dying. They’re almost impossible to recover.
Earlier treatment is key. We need to off-load the hospitals. We are tired. I can’t keep doing this. If you look at my manuscript and if I have to go back to work next week any further deaths are going to be needless deaths and I cannot be traumatized by that. I cannot keep caring for patients when I know that they could have been saved with earlier treatment and that drug that will treat them and prevent the hospitalization is ivermectin.
I am here today, I am calling to action, the NIH—their last recommendation was August 27th. August 27th. I want to be clear. I am not here as a politician, or a dramatist, or sensationalizing what I am recommending. I am going to be very clear and very simple. All I ask is for the NIH to review our data that we’ve compiled of all of the emerging data. We have almost 30 studies. Every one is reliably and reproducibly positive showing the dramatic impacts of ivermectin.
Please, I am just asking that they review our manuscript. It is a serious manuscript, by serious, highly experienced physicians and researchers. We have—I cannot call on more credibility than we have. We’re not just a random doctor who’s saying we have a cure. I don’t want to say I have a cure. I’m just asking, review our data. We have immense amounts of data to show that ivermectin must be implemented and implemented now.
Senator, the last thing I want to say, is, You know who’s dying here? It’s our African-American and Latino and elderly. It’s some of the most disadvantaged and impoverished members of our society. They are dying at higher rates than anyone else. It’s the most severe discrepancy I have seen in my medical career. And we are responsible to protect those disadvantaged members. We have a special duty to provide countermeasures. The amount of evidence to show that ivermectin is life-saving and protective is so immense and the drug is so safe, my colleagues have talked about it. It must be instituted and implemented. I am asking the NIH to review our data and come up with the recommendations for society. Thank you.
Ends at 0:38:12
Beginning at 1:01:21:
Senator Rand Paul:
Thank you, Mr. Chairman. I’d like to begin by apologizing for the juvenile diatribe from the Ranking Member. Science is about having an open mind. Science is about disputation, debate, evidence and it’s discussed. And the contention and the back and forth is how we determine what the truth is. But if you close your mind completely to this and are not willing to listen, I think that’s how science dies. That’s when we say, Well, the Government Consensus or the Scientific Consensus is this. That’s the closing of the scientific mind and that’s a recipe for disaster.
Science is also not about ad hominem and attacks. By attacking this panel without listening to it, leaving in a huff and having no questions shows a small-mindedness, a closed-mindedness and really it should be everything that we should avoid.
I’m not here to be an advocate for one treatment over the other and I will ask some tough questions to the panel. But I’m open-minded enough to listen to their side and see—and try to determine whether or not it’s a good treatment or bad. But to immediately close our mind, I think, is a bad way of looking at this.
I had a good friend die yesterday from this so I’m not one who’s saying this isn’t a deadly disease. She lived a couple doors down and we’re sad. Kelly and I are both sad about what happened. About six months ago we had a friend who died in their 30s. Not from the disease, but from lack of a Stress EKG. She died from a terminal arrhythmia in her 30s with two young children but her Stress EKG was canceled because the government decided that we shouldn’t do—it was an elective procedure. It was delayed and she died from a terminal arrhythmia.
So people also do die from the decisions that people make. The most important thing is is no one person is right. The panelists are not all right and people should question them and go back and forth and we try to figure out the truth from that.
But it’s a mistake to say one person should have all the power to determine what we should do when we place too much confidence in government doctors such as Dr Fauci. Dr Kory mentioned that he mentioned in June about steroids. I mentioned it in March when Dr Fauci came into my Committee Hearing. My first thought about the final pathway here with Covid in the end stages is not too dissimilar from other final pathways, Adult Respiratory Distress Syndrome.
I had a friend who is a surgeon who got the strep-eating flesh from operating on somebody who had it and a blood spatter, he got it. The chance of losing your limbs is like 50% to 70%. It’s like a 50% chance of losing all your limbs. It’s a devastating disease but one of the final common pathways, like Covid, is your blood vessels leak fluid into your lungs. It’s sort of a toxic shock kind of syndrome.
They treated him with high-dose steroids and so I raised my hand to Dr Fauci and said, Do you think steroids might have a role in this? He sort of dismissed me and said that the studies were showing that it probably wouldn’t work. But I would think most people would argue now that one of the most significant developments in the acute care of the Covid patient has been the steroids, actually, and trying to get them the steroids before they’ve gotten into the full ARDS syndrome. Some are even getting it at a very early stage in the disease.
But that came from people asking questions, being skeptical and not letting one doctor such as Dr Fauci say, Oh, that’s not right, young man, go sit in the corner. We need to have an open mind. I’m not saying I’m always right. I’m a bystander and I’m not an expert in Covid but I try to ask the important questions.
One of the questions that I’d like to ask, and I think this is the difficulty of proving the situation on either ivermectin or hydroxychloroquine is that because so many people get better, the control group, might be 99% of the people get better. Then you give hydroxychloroquine to the same group and you might get 99.5—it’s going to be a difficult thing to actually prove in trials that you get a benefit. It sounds like in some of the sicker patients where you had a mortality, you know, where you had a 25% mortality down to 15%, that does sound significant. Now you’re getting into the sicker patients.
With the outpatient studies, one of the critiques is that so many people get better naturally, how are you proving it’s statistically significant? What comes to my mind is, sort of like when we wanted to prove that taking an aspirin a day was good to prevent heart attacks, it took like 10 years and 10,000 people in the study because it was just hard to show the differences of whether an aspirin worked or not. I think the same thing is true with either hydroxychloroquine or ivermectin in an outpatient setting, is that because so many people get better on their own the converse is when you’re sick because it’s hard to treat people who are very sick. It’s hard to prove that anything works when people are very sick.
I guess what I’d like to do is open it for the panel, one by one, to explain how we answer the critique that most of these people are getting better anyway, so how are you proving your treatment works in a group of people who didn’t go to the hospital so that you were selecting out actually for the people who may well have been—you know, did you prevent them from getting seriously sick or have you selected out as your patient pool because they’re outpatient, tending people who would get better? We’ll start with those who are here.
Beginning at 1:08:48:
Dr Kory:
Senator Paul I appreciate your question and it’s critical, the content of your question which is how can we tell when something’s working when many patients get better? There’s only one answer to that. We know what that is and it’s one of the central tenets of science, which is you need a control group. You need to have a group that is comparable to those that you treat and then you compare them to those you don’t treat.
What I am trying to message today is in our manuscript, we now have 11 randomized control trials. Every one of those control trials show that in the ivermectin treated group, lives are saved, there’s less need for hospitalization, there’s less transmission, less case counts. It is a fundamentally and powerfully effective therapy against covid-19. We need the NIH to review these data. We have the data.
Let me say, the amount of patients in those randomized control trials, the 11 trials total, nearly 4,000, with over half treated with ivermectin. Let’s remind ourselves that the treatment of covid-19 fundamentally changed after the recovery trial was announced in June. That was a trial of 6,000 patients. 2,000 were treated with steroids and it showed the dramatic and life-saving property of corticosteroids. Almost overnight the treatment of covid-19 changed as a result of that trial. That was the recovery trial.
I am presenting a paper today with more patients treated with ivermectin. With larger magnitudes of benefits in the recovery trial. I will maintain ivermectin should be the standard of care of this disease based on these data. It’s not be my opinion. It’s the data. We have the data. If you give anyone else a placebo based on the data that’s in our manuscript, I believe that would be malpractice and you would lead to the heightened risk of death. No more placebo is needed.
Beginning at 1:50:51:
Senator Johnson:
I’m a big supporter of allowing doctors to be doctors and allowing patients to make these decisions because it’s their lives, it’s their family’s lives. We talked about other world bodies or other things that are happening globally. In our last hearing, Dr McCullough pointed out that the death rate in India is about 95 per million. In the U.S. and other ‘advanced’ nations, it’s close to 800 per million. I’m not sure who to direct this question to, but are you aware of us actually studying what these other countries are doing? One thing I’ve been struck [by] is I’ve been kind of tipping the spear here so I get a lot of information. I’m not a doctor, but it’s an awful lot of interesting information. And one of the things that i have found out or heard is some of these less developed countries that don’t have the type of money to throw at a medical system like the U.S., all they have are these cheap, generic drugs, are using them and doing quite well. Does anybody have some expertise to kind of speak to that? ...
Beginning at 1:53:55: Senator Johnson: Dr Kory.
Dr Kory: Senator, my organization, the Front Line COVID-19 Critical Care Alliance, we’ve worked with a number of analysts. Two analysts that are part of our organization have been doing numerous epidemiologic analyses throughout the pandemic. Their data, which again I have to say is free to share, we can share with the NIH, the FDA so they can evaluate the data. If I can go through that data very briefly, I would appreciate it. I brought slides. I will go through them very quickly. They are visual and easy to understand.
Senator Johnson: Is this the one on Peru?
Dr Kory: Yes, and let’s start with that, because Dr Bhattacharya just mentioned something is that one hypothesis is they’re younger generations. I have data to show that’s not true. Number one, this is only in patients over 60. We know the mortality rates in patients over 60. They are fundamentally different than in younger patients. When you only look at patients over 60 and you look at this slide, this is in the eight regions of Peru, eight states in Peru that initiated ivermectin distribution campaigns throughout their population.

If you look at each graph, the shaded area to the left of the graph is before the ivermectin distribution. To the right of that shaded area is after they initiated ivermectin distribution campaigns. In each of eight states you see what we call a temporally associated reduction. There is a peak in death, a peak in case counts and a peak in case fatality rates which rapidly decrease to pre-pandemic levels. This is powerful, powerful data. If you could go to the next slide. The next slide, I believe, if you can show me, that’s actually a skip, but I’ll say this has been replayed. We have data from many, many countries. On our website our analysts have numerous examples. This is one in Paraguay.

There was a state in Paraguay called Alto Paraná. The Governor there got covid. His brother got covid. They took ivermectin and felt immediately better and so they concluded that ivermectin was an effective treatment. I’m not saying that’s how we determined treatments but that’s what they did. The Governor did something really dramatic. He immediately began what he called a Deworming Campaign throughout his state because he didn’t want to go against the Federal Health Ministry which was against ivermectin. In his state he began to distribute ivermectin to the population. If you look at the graph, —
Senator Johnson: That’s the blue line.
Dr Kory: —the case count in deaths peak and they rapidly decrease. A month and a half later, he found almost no cases in the hospitals. That was in Paraguay. If you can go to another slide, I can show—are there any more slides that you have?
Senator Johnson: This is the one in Mexico.

Dr Kory: This is deaths in Mexico. The left side of the graph is before August 1st and the right is after. The green-shaded state is the is the state of Chiapas in Southern Mexico. That state, alone among all the states in Mexico, decided to incorporate ivermectin in its treatment protocols and if you look, the case counts—and these are widely available and globally used databases of case counts and deaths—you can see the deaths plummeted, while in all the surrounding regions in Mexico the deaths either decreased only slightly or in the majority they increased.
So you’re seeing this play out on population-wide basis in many regions of the world. There’s another slide. Please advance.

Here, going back to Peru: if you look at the blue lines and graphs, those are those eight states that I presented whose Regional Health Ministries decided to widely distribute ivermectin. The red bars refer to Lima, the biggest city in Peru. Guess what happened in Lima? The Health Ministry of Lima did not employ ivermectin in the treatment of COVID-19 and if you can see, throughout the summer and throughout this pandemic the case counts rapidly rise and remain high and only recently have come down but they’re nowhere near the regions in which ivermectin was widely used.
We have this data. It’s showing that we have an effective treatment against this pandemic. I cannot overemphasize that.